|
|
Dyop® - Dynamic
Optotype™ Helping the world see clearly, one person
at a time. |
|||||||
|
|
||||||||

Vision Scientists and Eye Care Professionals
have known for decades -
that the Snellen test is inaccurate and
inconsistent.
|
"Results
confirm the arbitrary nature of the Snellen fraction and warn about
the accuracy of visual acuity determined by using charts of different letter
types, calibrated by Snellen's system." A. Medina, B. Howland - Ophthalmic
and Physiological Optics, January 1988 “A
novel high-frequency visual acuity chart” https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1475-1313.1988.tb01076.x The
Dyop® test optimize the refraction and acuity processes to generate a more
precise and consistent refraction to reduce
both patient and refractionist visual stress. In an era where Smartphones and computers
are ubiquitous, the errors inherent in Snellen testing are no longer
acceptable. Preliminary studies
indicate that Dyop® acuity tests: · are more accurate (up to 6x) than Snellen/Sloan tests, · are more consistent (up to 8c) than Snellen/Sloan tests, · are potentially faster (up to 3x) to use than
Snellen/Sloan tests, · maintain greater precision as refractive power increases, · inherently avoids overminused and underminused
refractions, · minimize optotype fixation and decision fatigue, · minimize image memorization, · do not require the ability to read to measure visual
acuity, · allows for precise color acuity measurement for potential
diagnostic and therapeutic applications. · potentially save doctors and patients’ time and money in
determining visual needs. · consistently evoke 0.25 to 0.50 diopters of less minus refractive
power than Snellen testing. Clinical
results demonstrate improved Dyop precision, consistency, efficiency, and
reduced excess minus. https://www.dyop.info/documents/Snellen_vs_Dyop_Refractions-Sanni.pdf https://www.dyop.net/documents/ASOP-2022-01_Sanni-update.pdf Gordon
Paper – Pre/Post Cataracts https://www.dyop.net/documents/JCOVS-21-Gordon_refraction_comparison.pdf https://www.dyop.net/documents/Guy_Barnett-Itzhaki_The_Dynamic_Optotype.pdf Dyop® acuity tests are
intended to be a more precise and faster to use replacement for Snellen,
Sloan, and Landolt visual acuity/refraction tests.
Dyop® tests use
apparent motion detection from the strobic stimulus and
refresh rate of the photoreceptors to determine the visual acuity and
refraction endpoints. Snellen letters are culturally
derived, NOT proportional, and do NOT provide
a consistent basis for determining visual acuity. As a
result, Dyop® tests are more accurate and
efficient than the 1862 classic Snellen test, and
create a visual acuity test based on physiology rather than subjective
and imprecise cognition. Dyop® tests
enable patients to have a visual acuity endpoint which avoids overminused
refractions which seem to be inherent with static image
fixation. It is typically difficult for patients to perceive when
optotypes are "too crisp" (over- minused), despite the discomfort
and visual stress, which is one of the inherent inadequacies with Snellen and
other static image tests. Dyop® tests
determine visual acuity based upon photoreceptor
physiology with a
precision (approximately +/- 0.04 diopters) not previously available
with traditional static image visual acuity tests. Unlike static
image tests, which may be dependent upon cognition as much as they are for
visual acuity, Dyop® tests also maintain a higher
level of accuracy as visual acuity decreases with increased blur.
Is 1862 Vision Technology Making 21st Century Patients
Blinder? The Dyop strobic stimulus has greater
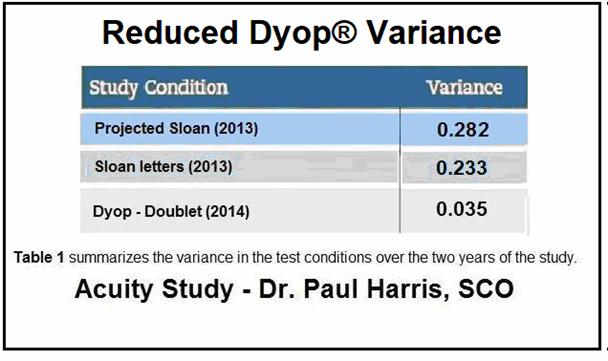
precision and less variance than static visual targets The increased precision and consistency and “resolution
acuity” of Dyop tests are intended as a global replacement for static
letter-based “recognition acuity” tests such as Snellen, Sloan, and
Landolt optotypes, and can provide a more universal and efficient
method of vision measurement.
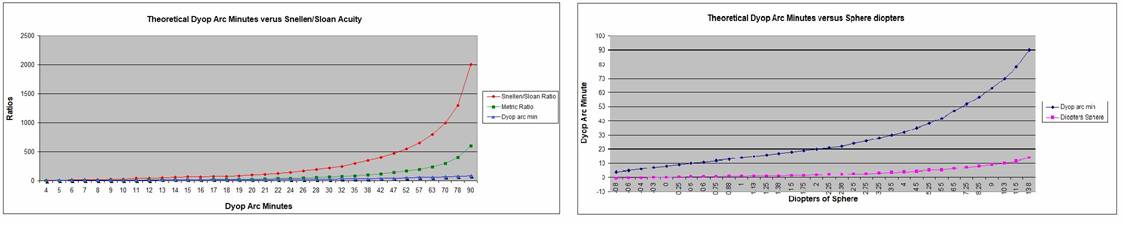
The 2013 projected Sloan optotypes are
“fuzzier” than the 2013 computer generated Sloan optotypes, and thereby give
a “fuzzier” acuity response. The 0.54 arc minutes squared Dyop® visual
stimulus area (the arc width of the gap/segments) is smaller and inherently
more precise than the 1.0 arc minute squared visual stimulus area (the
“Minimum Area of Resolution”) of Snellen/Sloan/Landolt optotypes. The
0.54 arc minutes squared Dyop® visual stimulus area correlates to about 20
photoreceptors.
Fixating on static Snellen/Sloan images also increases
accommodative stress, which leads to an overminused acuity response and
possible overminused refraction. The visual dissonance/stress
from an overminused refraction is frequently a major reason for
patients’ complaining about their lenses and/or not wearing their lenses at
all.
The Dyop® Acuity/Refraction Test can
be used on virtually any personal computer system with minimal setup-up and
training. Dyop® vision testing should increase the accuracy of
prescriptions, let patients more easily know when their vision is not proper,
maintain higher practitioner testing consistency, and potentially save
doctors and patients’ time and money when getting their vision checked. |
|||||||||||||
|
The Dyop® concept
is revolutionary, both literally and culturally. Previous static
methodologies for measuring visual acuity were culturally based and a
combination of the perceptual guesses of the subject and the observational
guesses of the examiner. The 1862 Snellen test, and the 1888
Landolt ring as an attempt at a “culturally neutral” test, use static images
with a limited precision increment range that is no longer adequate for a
society where much of the day is spent looking at the precision of a computerized
display and/or regularly travelling at speeds greater than 55 miles per hour
(88.5 kilometers per hour). Snellen letters are culturally
derived, NOT proportional, and do NOT provide
a consistent basis for determining visual acuity: Snellen
tests also ignore the fact that the visual stimulus is the “Minimum AREA
of Resolution” rather than the “Minimum ANGLE of Resolution.” Visual
acuity measurement in increments of +/- 0.25 diopters was acceptable and
adequate in 1862 because of the difficulty of making lenses more precisely
than +/- 0.25 diopters. Visual testing in increments of +/- 0.25
diopters was also adequate because of the small percentage of the population
able to read, or needed to be able to read. Varying
Difficulty of Snellen Letters and Common Errors in Amblyopic and Fellow Eye PDF File https://archopht.ama-assn.org/cgi/content/abstract/129/2/184 https://archopht.jamanetwork.com/article.aspx?articleid=426887 Snellen
test responses also are NOT equivalent to the responses from
the academically preferred Landolt ring test. Because of the increased cognition factor inherent
in the non-uniformity of the Snellen letters, for them to be equivalent
to the 5 arc minute size of Landolt rings, Snellen
letters should actually be only 4.25 arc minutes in size (15% smaller) and
NOT the currently accepted 5.0 arc minute height. Correlation of Optotypes with the Landolt
Ring PDF
file PDF
file Note: Dyop® tests are
for vision screening purposes only and are NOT a
substitute for an examination by a licensed vision care
professional. |
The Dyop® (Dynamic Optotype™)
tests and concept are covered under U.S. Patent US 8,083,353
and International Published Patent WO
2011/022428.
For further information contact: Allan Hytowitz
at Allan@DyopVision.com
5035 Morton Ferry Circle, Alpharetta,
GA, 30022 / 404-281-7798
Copyright©2023 DyopVision™ Associates. All Rights Reserved.