|
Introducing
the Dyop® The
“Revolutionary” Method for Measuring Visual Clarity (Acuity) Helping the world see more clearly, one person at a time.
Vision is an autonomic and dynamic
process inherent in all animals because the world we see is dynamic, rather
than static. Our eyes are biological
machines which help us survive by enabling us to automatically detect motion, distance, and colors
so that we can see predators and food and eat rather than being eaten. By being autonomic most of us don’t have to
think about what it would take to have things we see be properly in focus. Visual acuity is the term used to describe the clarity of what
you see. A refraction
is the process of using special lenses to measure optical variables of sphere,
cylinder, and axis which go into creating eyeglasses and contact lenses
and compensate for “less than perfect” vision. Typical vision tests use static letters
or symbols as the standard targets for measuring vision. The flaw in those static measurement systems is that they typically
measure only two dimensions using
the height of the visual target and the viewing distance to
that target. Instead, the world we see
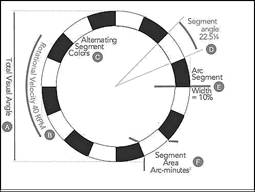
is a fifth dimensional process consisting of height, width, colors, distance, and time. A Dyop® (pronounced “di-op” and short for dynamic optotype) is a calibrated segmented spinning ring visual target
(aka, optotype) which helps doctors (and you) test how clear your vision
is. A Dyop provides a dynamic strobic stimulus (DSS) = = = = = = = =
= = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = =
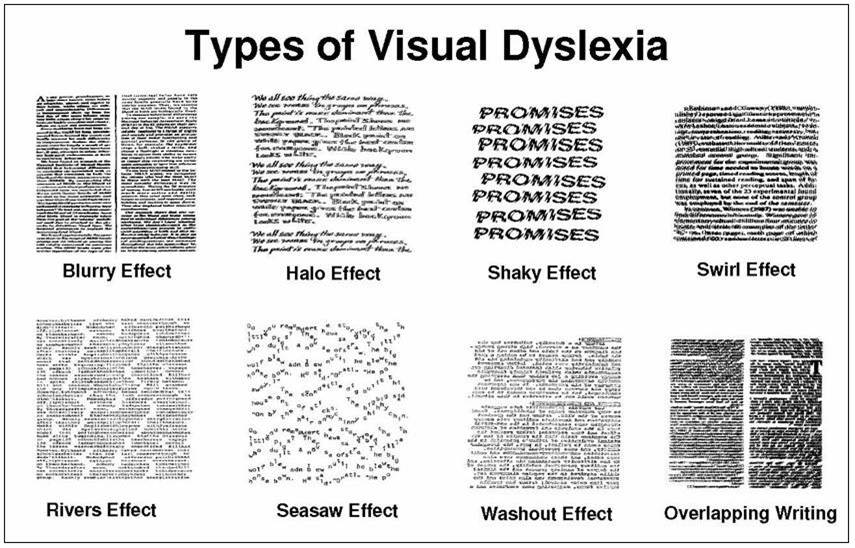
= = = = = = Recent Dyop Discoveries Recent Dyop discoveries have compared inaccurate
refractions, and the effects of cataracts, to the reduction of cognition
associated with dyslexia. Induced Dyslexia: https://www.dyop.net/documents/Induced_Dyslexia.pdf That analysis and refraction
research also explains why the current Global Epidemic of Myopia may likely be a result of the use of the
current computerized Snellen test for refractions with its white computer-generated background, functioning to
burn out the response of the fovea photoreceptors. The ORIGINAL format of the 1862 Snellen
test used black letters on white paper and reflected light to make the black
letters visible and identifiable. https://www.dyop.net/documents/How-Snellen-Computerized-Vision-Testing-is-Adding-to-Myopia.pdf = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = =
= = = = = = = = = = = = = = = = = = For vision to be effective and efficient, it needs to be autonomic (so
that we are unaware of that process). However, acuity
is NOT regulated by the brain.
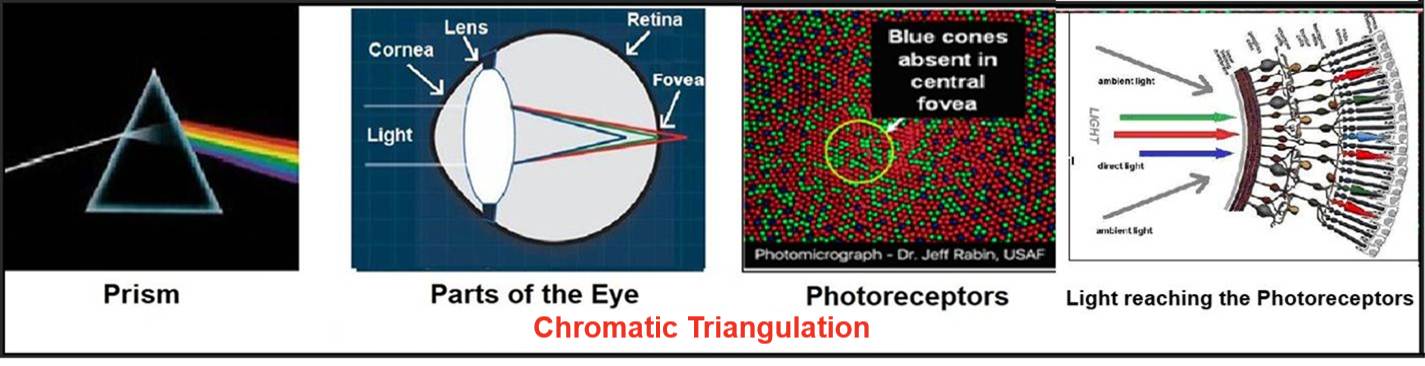
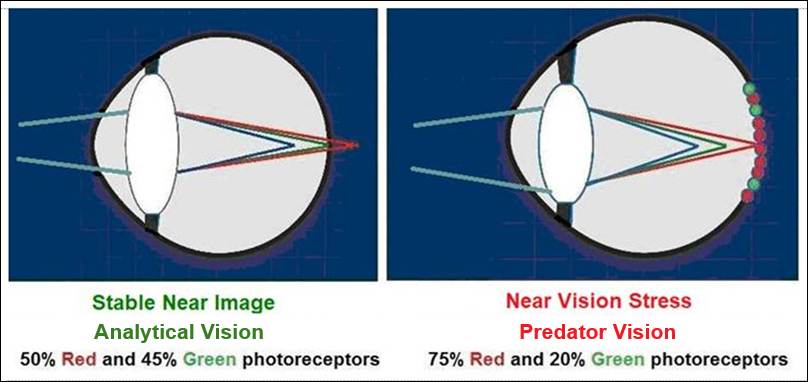
As
light goes through the cornea and lens, it is bent (refracted)
so that Blue is focused in FRONT of the retina, Green is focused ON the retina, and Red is focused BEHIND the retina. (See the diagram below.) Acuity is regulated by the relative focal
depths and intensity of those three colors in a process called Chromatic Triangulation as the intensity of those colors is
perceived by the color sensitive cone-shaped photoreceptors in the back of
your eye (called the fovea). A Dyop functions as a visual
equivalent of an Audio Tuning Fork. An Audio
Tuning Fork provides an auditory tone that can be
used to calibrate other sounds. The strobic stimulus of
a segmented spinning Dyop ring and Chromatic Triangulation functions as a Visual
Tuning Fork to regulate the focal depth of a
visual image by adjusting the shape of the biological lens to keep the visual
target in focus based on the relative focal depths of the colors
of Blue, Green, and Red that comprise the image.
Chromatic Triangulation is based on the
concept of bending (refracting) light that Isaac Newton discovered in 1665
when he filtered light through a prism. To regulate acuity
(visual clarity), clusters of 20 color sensitive cone-shaped
photoreceptors (creating a stimulus area of 0.54 arc minutes squared for
20/20 or 6/6 acuity) and send their stimulus signals forward (based on
the relative intensity of those specific wave-length colors) to the layer of
neuroganglia in front of the retina. That neuroganglia layer of
cells (functioning akin to a biological circuit board) then sends a signal
from those clusters of 20 photoreceptors to the cilia surrounding the
lens to regulate the lens shape and keep that image in focus. Simultaneously, the combined signal of 100
adjacent fovea photoreceptors is sent from the neuroganglia to the brain
via each optic nerve fiber to record that image. The process of
combining the response of the color-sensitive photoreceptors to light and
color is akin to the pixel images you see on
your computer monitor, tablet, or Smartphone. You think you are seeing lines, shapes,
letters, and/or words. What you really are seeing are
pixels of light moving rapidly across the surface of your
computer screen, tablet, or Smartphone in
combinations of Red, Green, and Blue. The process of acuity regulation and
accommodation by the color receptive cone-shaped photoreceptors to bring the
focus of light onto the retina we call Chromatic Triangulation.
Chromatic
Triangulation https://www.dyop.net/documents/Dyslexia_and_Color_Perception-SandraStark.pdf https://www.dyop.net/documents/ASOP-06-0651-Dyop_Color_Perception.pdf = = = = = = =
= = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = =
= = = = = = = A simple
experiment to demonstrate and validate that acuity is NOT regulated by the brain but rather is regulated using Chromatic Triangulation of
the colors Red, Green,
and Blue using the color sensitive photoreceptors in the
fovea of the retina. Close one eye and
look around the room where you are now. You will notice that with only
one eye open you can still determine
the relative distance to nearby objects without the need for binocular vision documenting that acuity
is NOT regulated by the brain. If you
wear glasses, a simple test to also verify that your
lenses are too strong (typical of
Snellen refractions which have too much minus power IF you wear glasses), is
to push your glasses about a half inch away from your face and see if the
words you are reading become larger and more legible. If you notice
that the words get more legible, that indicates that the Snellen-induced
excess minus power of your glasses is typically about 0.25 to 0.50 diopters.
While it isn’t much, it reduces your cognition and possibly your IQ by 10 or
more points. You can
also verify the hyper-stimulus visual effect of the bright white background
of a typical computer-generated static-image vision test (e.g., Snellen) by
briefly staring at a white light bulb and then closing your eyes. With
your eyes closed you should notice a white stimulus ring for an additional
ten seconds from your depleted retina photoreceptor response. The
similar computer-generated hyper-stimulus of the
WHITE background with Snellen and other
static vision tests is a probable
contributor to the visual damage (typically an excess -0.50
diopters of sphere) from using Snellen testing. Snellen
testing is likely a major factor in the Global Epidemic of Myopia of the past forty years concurrent with the advent
of computerized vision testing. = = = = = = =
= = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = =
= = = = = = = NEAR Vision
Stress (an Unstable NEAR Image) is typically associated with
dyslexia, migraines, and epilepsy, however, those individuals also tend to
have a Stable DISTANCE Image.
Those individuals with NEAR Vision Stress typically have a lower percentage of Green-sensitive photoreceptors
(only 20%) versus Red-sensitive photoreceptors
(75%) in the rear
fovea area of the retina making it more difficult to keep the lens in proper
focus for near images. The
evolutionary advantage of that Stable DISTANCE Image (20% Green and 75% Red) is that it enabled
humans to be better at spotting predators and game. As human culture (and biology) evolved from using drawings on the walls
of caves as a primary form of written communication, to pictographs
representing sounds and images, and then evolved to using symbols as
representatives of letters and sounds which were combined as words, the
benefits of a Stable Near Image (45% Green and 50% Red) versus the
original a Stable DISTANCE Image (20% Green and 75% Red) increased
because it allowed greater creativity and flexibility in dealing with
concepts and enhanced the use of technology.
(Technology is defined as the use of information as a substitute for
time, energy, and matter.)
Unstable
NEAR Image
versus Stable Near Image Stable DISTANCE Image versus Unstable DISTANCE Image
As the benefits of using written words as a skill increased the
survival and technical advantage for dealing with predators and game, the
problem with those individuals who have an Unstable NEAR Image became
identified as dyslexia.
Other
side effects of an Unstable Near Image
are migraines and epilepsy. An Unstable Near Image is
also a contributory factor in PTSD (Post
Traumatic Stress Disorder), making
recovery and dealing with PTSD more difficult. = = = = = = = = = = = = = = = = = = = = = = = = = = =
= = = = = = = = = = = = = = = = = = = = = = = = = = How
Acuity is Measured The
properties of visual clarity (acuity) are the SIZE (area) OF THE IMAGE being observed, the VIEWING
DISTANCE to that image, and the
ability of the visual system to PROCESS THAT IMAGE as clearly as possible (Resolution
Acuity). As a Dyop® spinning ring gets smaller, the
(equally sized) gaps and segments become so small that it becomes impossible
(sub-acuity) for the eye to detect the spin direction of the Dyop ring rotation. The Dyop acuity endpoint is the smallest Dyop diameter where the direction
of rotation of the spinning ring can still be detected. It serves as a precise, physiological
indicator of visual clarity and vision correction. A Dyop test can measure
vision without the need for patient literacy, measure vision
in infants as young as 14 months of age and let doctors precisely
measure vision in color enabling potential diagnostics for symptoms of
dyslexia and glaucoma. https://www.dyop.net/documents/Dyop_Infant_Acuity_Measurement_Poster.pdf
Static acuity tests (such as Snellen letters)
are inherently imprecise and inconsistent using Recognition Acuity.
It mistakes the process of visual cognition for visual resolution
and uses an arbitrarily determined and overly large stimulus area (1.0 arc
minutes squared) as the benchmark for vision rather than the empirically
determined smaller Dyop stimulus gap area (0.54 arc minutes squared). Additionally, computer-generated static vision tests such as Snellen deplete the
dynamic response of the color receptive photoreceptors in the fovea and lack
the uniform precision of Dyop testing.
The result is that static vision tests tend to add excess minus power
(about 0.5 diopters) to acuity and refractions, lead to angular elongation of the eye and
increased myopia, and indicate that Snellen testing itself may now be a factor in the Global Epidemic of Myopia. https://www.dyop.net/documents/Snellen_vs_Dyop_Refractions-Sanni.pdf https://www.dyop.net/documents/ASOP-2022-01_Sanni-update.pdf A simple test to verify that your lenses are too strong with too much minus
power (IF you wear glasses), is
to push your glasses about a half inch away from your face and see if the
words you are reading become larger and more legible. If you notice that the words get more
legible, that Snellen-induced excess minus power of your glasses is typically
about 0.25
to 0.50 diopters. While it isn’t much, it does reduce your
cognition, and possibly your IQ by 10 points.
(See Acuity Validation above.) Using a Dyop for testing
vision is better than the use of static letters (aka, the 1862 Snellen’s
“Big E” test) or static shapes because the dynamic/spinning strobic stimulus of a
Dyop is based on how your eyes work. As the Dyop diameter gets smaller, its
alternating gaps and segments get proportionately smaller. When the spinning Dyop gaps get sufficiently
small, the stimulus area of each gap becomes smaller than the minimum AREA to
stimulate the color-receptive
photoreceptors in the rear (fovea) area of the retina, which are clusters of
about 20 color-receptive photoreceptors.
When the Dyop gaps become too small to sufficiently stimulate a
cluster of photoreceptors, the spinning of the Dyop ring is
not detected because the stimulus of
the gaps and segments tend to merge. A
Dyop NOT detected as spinning is a “sub-acuity” diameter. As the Dyop diameter
is increased to enable the gaps to
stimulate a minimum of 20 fovea photoreceptors, that minimum Dyop diameter
where spinning IS detected
becomes the Acuity Endpoint. That minimum size threshold for
detecting the gaps as spinning is also called the Minimum AREA of Resolution (MAR). A
major flaw in current letter-based acuity testing, and acuity “standards”
using letters is that Snellen acuity is a two-dimensional system dealing only
with letter height and viewing distance and (mistakenly) as the “Minimum ARC of Resolution” rather than the “Minimum AREA of Resolution.” The result of using Dyop Resolution
Acuity for
acuity and refractions is that a Dyop is up to six times more precise than the 1862 derived Snellen
static letter-based tests (which use culturally dependent static Recognition Acuity letters or
symbols), is up to eight times more consistent, and is up to three times more efficient. A Dyop also can measure acuity regardless of the subjects’ literacy skills or culture, easily enables testing of children or infants, and enables
measurement of acuity in color for potential diagnostic and/or therapeutic
use. https://www.dyop.net/documents/Dyop_Infant_Acuity_Measurement_Poster.pdf And because a Dyop can measure acuity in color, it also enables the
realization that, for most humans, color is an essential part of being able
to see and regulate acuity. Static vision tests
(e.g., Snellen) are based on how well you recognize culturally dependent
letters or symbols using Recognition Acuity, are influenced by where you're from, or how much
you've practiced (or memorized) the Snellen test, and are intentionally only
in black and white even though most people see in color. Using Resolution Acuity with a Dyop
makes vision testing simpler, faster, more precise, and more consistent. = = = = = = = = = = = = = = = = = = = = = = = = =
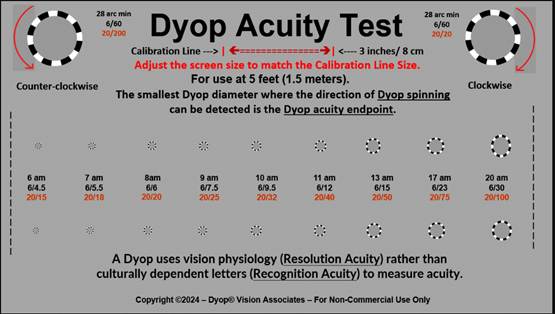
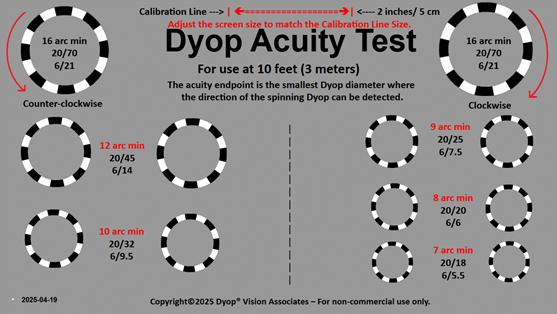
= = = = = = = = = = = = = = = = = = = = = = = = = = = = Online Dyop Visual Acuity Tests Select the link below to access the
visual clarity (acuity) test for the correct viewing distance. View the spinning rings at a five-foot or
ten-foot distance. Note the smallest pair of Dyop rings you
can detect as spinning. The center row of numbers between the
smallest pair of rings you can detect as spinning rings is the measure of your acuity. (Below are static images of the Dyop
online Acuity test.)
Dyop
Acuity Screening
Test for use at 5 feet Dyop Acuity Screening
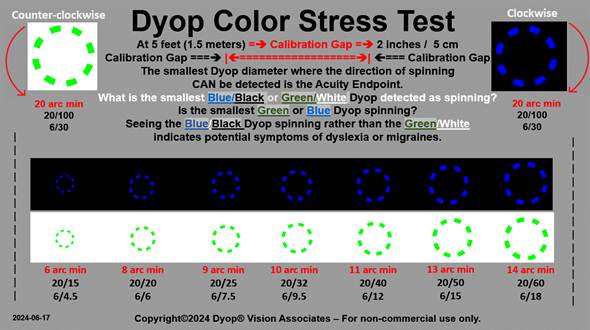
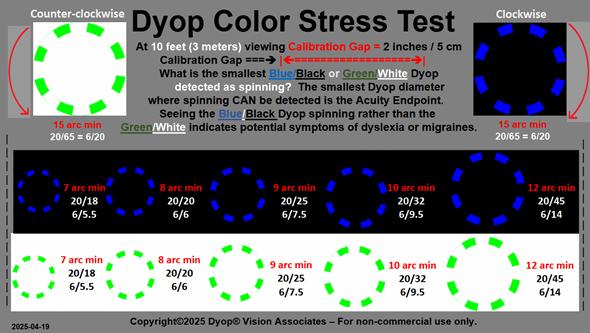
Test for use at 10 feet Online Dyop Color Stress Screening Test Select the link below for the color screening (visual stress) test for the
correct viewing distance. View the spinning rings at a five-foot or
ten-foot distance. The
smallest colored Dyop ring (Blue/Black or Green/White) you can detect as
spinning indicates your color
acuity profile. Preferentially seeing
the Blue/Black rather than the Green/White indicates a probability of
symptoms of dyslexia, migraines or epilepsy. The center row of numbers between the
smallest rings you can detect as spinning is the measure of your color
acuity. (Below are static images of the Dyop
online Color Stress Screening test.)
Dyop Blue/Green Visual Screening Test – 5 feet - - - - Dyop Blue/Green Visual Screening Test – 10 feet = = = = = = = = = = = = = = = = = = = = = = = = =
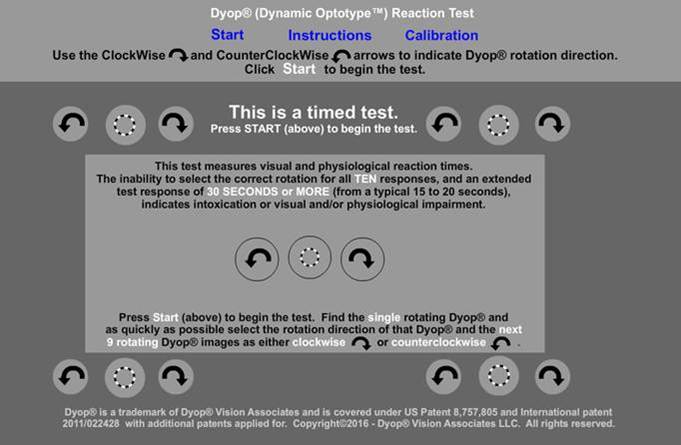
= = = = = = = = = = = = = = = = = = = = = = = = = = = = Dyop Cognition-Impairment Test A Dyop may also be
used to evaluate the visual and mental impairment associated with conditions
such as marijuana
intoxication, PTSD, concussion injuries, and other possible mental
difficulties such as Alzheimer’s. https://www.dyop.net/documents/Dyop_Cognition_Test.html Use the link above to open the Dyop
Cognition-Impairment test. Note that THIS is a Timed Test. Click the word “Start” at the top of
the test to begin. Additional details are at: https://www.dyop.net/impairment.htm (Below is a static
image of the initial screen for the Dyop Cognition-Impairment
Test.)
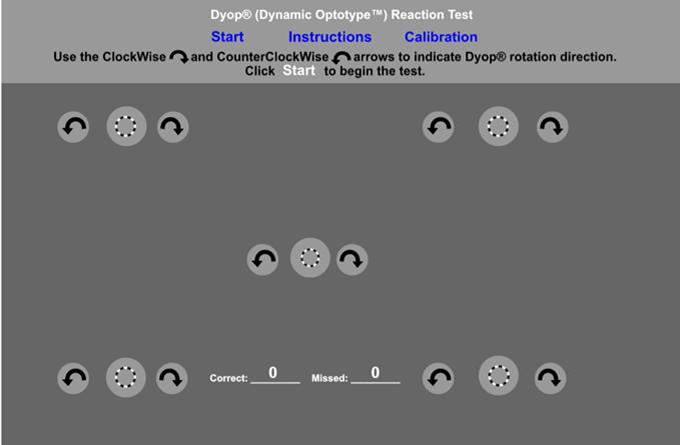
Note that when the test starts, there will be FIVE
Dyops on the screen but only ONE of them is spinning. Use a computer mouse or touch screen to click the
arrow adjacent to the SINGLE spinning Dyop to indicate its spin direction. That Dyop will stop spinning, but ONE of the other
FOUR Dyops will then start spinning. Click the arrow adjacent to that next spinning Dyop
to indicate its spin direction. (Below is a static image of the response screen for
the Dyop Visual-Impairment Test.)
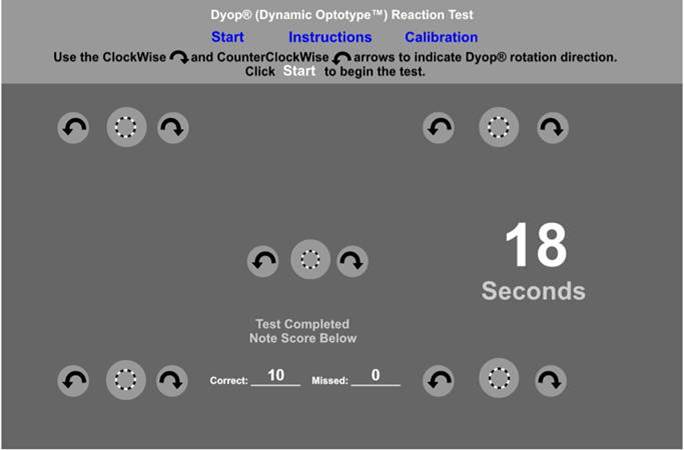
When you have found and detected all TEN of the
spinning Dyop test response trials, the screen will display the number of Correct Selections and
the elapsed Test Time. A test completion time of 14 to 16 seconds with 10
correct responses indicates mental alertness. A test completion time of 21 to 26 seconds with less
than 10 correct responses indicates minor mental impairment. A test completion time of 28 to 32 seconds with less
than 8 correct responses indicates increased mental impairment. A test completion time of 35 to 40 seconds with less
than 6 correct responses indicates significant mental impairment. (Below is a static image of a typical final response
screen for the Dyop Visual-Impairment Test.)
= = = = = = = =
= = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = =
= = = = = = The Dyop® (Dynamic Optotype™) tests and concept are covered under U.S. Patent US 8,083,353 and International Published Patent WO 2011/022428. for further information contact: Allan
Hytowitz at Allan@Dyop.org 5035 Morton Ferry Circle, Johns Creek,
GA, 30022 / 404-281-7798 Copyright©2026
DyopVision™ Associates. All Rights Reserved. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}